We are now "Susan At Antonino Salon" specializing in Human Hair, Human Hair/Synthetic Blend and Synthetic wigs. I am an Oncology Nurse and Breast Cancer Survivor offering products for women undergoing Chemotherapy and Radiation Treatment since 1994. “The Fit of Custom Made. The Value of Custom Tailored.”
CALL or TEXT 248-544-4287 for your FREE consultation on Monday and Tuesday from 10 AM to 4 PM. We are located within Antonino Salon, 191 Townsend, Birmingham, MI 48009.
Thursday, April 26, 2018
The Mayo Clinic Breast Cancer Book
The essential guide to breast cancer
Whether you are facing a cancer diagnosis and the challenges of treatment, or wish to prevent the disease if you're at high risk, this book brings you the most accurate, reliable and up-to-date information available.
You'll discover a story rich in hope, with accounts of women who've successfully confronted this difficult disease.
The knowledge you'll gain will help you be a more informed patient — in communicating with your doctor, in selecting among treatment options. In 453 pages of thorough coverage, Mayo brings you critical knowledge in many key facets of breast cancer.
Prevention — What can you do to decrease your risk of getting breast cancer? While there's still no guaranteed way to prevent it, several lifestyle factors can be modified to reduce your risk, especially if you are in a high-risk category.
Treatment — After diagnosis comes a flurry of questions: "Now what?" "How do I deal with this?" "Do I have options?" "What's my prognosis?" The good news is that breast cancer is now considered a highly treatable disease with good results. Survival rates keep increasing. The book reviews the full range of treatment options, and the pros and cons of each.
Care and Coping — Life goes on after diagnosis. Our doctors share their best options for dealing with feelings and emotions ... for coping with treatment side effects ... for women who want to consider complementary therapies. A separate chapter offers helpful guidance to the patient's partner.
Living With Hope — It bears repeating: Breast cancer is highly treatable. You have every reason to live with hope. This book offers key support for every woman.
The book is a tribute to many, especially the extraordinary women who've taught us about breast cancer. Each has added to our knowledge of the disease, and advanced your ability to respond to any diagnosis or risk.
Our 100% Money-back Guarantee We are confident you will find great value in the informational products published by Mayo Clinic. If you are not completely satisfied, you may return your order within 30 days for a full refund.
Once you've been diagnosed with breast cancer, your doctor will review your pathology report and the results of any imaging tests to understand the specifics of your tumor.
Using a tissue sample from your breast biopsy or using your tumor if you've already undergone surgery, your medical team determines your breast cancer type. This information helps your doctor decide which treatment options are most appropriate for you.
Here's what's used to determine your breast cancer type.
In what part of the breast did your cancer begin?
The type of tissue where your breast cancer arises determines how the cancer behaves and what treatments are most effective. Parts of the breast where cancer begins include:
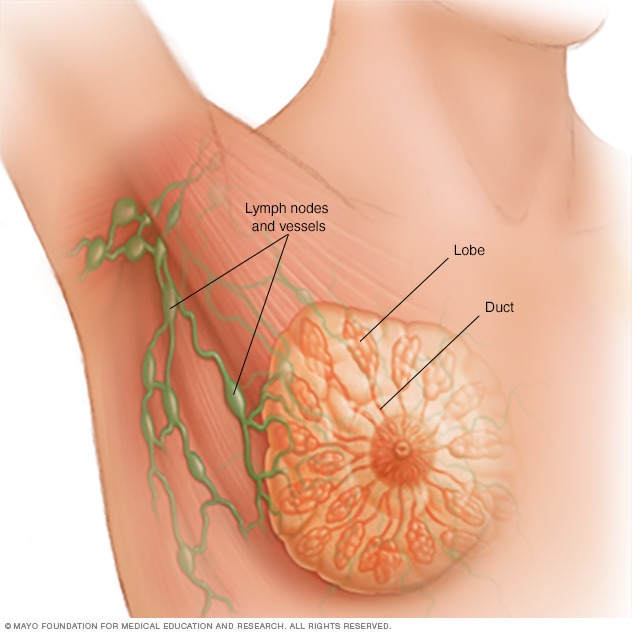
Milk ducts. Ductal carcinoma is the most common type of breast cancer. This type of cancer forms in the lining of a milk duct within your breast. The ducts carry breast milk from the lobules, where it's made, to the nipple.
Ductal carcinoma can remain within the ducts as a noninvasive cancer (ductal carcinoma in situ), or it can break out of the ducts (invasive ductal carcinoma).
Milk-producing lobules. Lobular carcinoma starts in the lobules of the breast, where breast milk is produced. When it breaks out of the lobules, it's considered invasive lobular carcinoma. The lobules are connected to the ducts, which carry breast milk to the nipple.
Connective tissues. Rarely breast cancer can begin in the connective tissue that's made up of muscles, fat and blood vessels. Cancer that begins in the connective tissue is called sarcoma. Examples of sarcomas that can occur in the breast include phyllodes tumor and angiosarcoma.
How do your cancer cells appear under a microscope?
When a sample of your breast cancer is examined under a microscope, here's what the pathologist looks for:
Cancer cells with unique appearances. Some subtypes of breast cancer are named for the way they appear under the microscope. Subtypes include tubular, mucinous, medullary and papillary. Your subtype gives your doctor some clues about your prognosis and how your cells may respond to treatment.
The degree of difference between the cancer cells and normal cells. How different your cancer cells look from normal cells is called your cancer's grade. Breast cancers are graded on a 1 to 3 scale, with grade 3 cancers being the most different looking and considered the most aggressive.
Are your cancer cells fueled by hormones?
Some breast cancers are sensitive to your body's naturally occurring female hormones — estrogen and progesterone. The breast cancer cells have receptors on the outside of their walls that can catch specific hormones that circulate through your body.
Knowing your breast cancer is sensitive to hormones gives your doctor a better idea of how best to treat the cancer or prevent cancer from recurring.
Hormone status of breast cancers includes:
Estrogen receptor (ER) positive. The cells of this type of breast cancer have receptors that allow them to use the hormone estrogen to grow. Treatment with anti-estrogen hormone (endocrine) therapy can block the growth of the cancer cells.
Progesterone receptor (PR) positive. This type of breast cancer is sensitive to progesterone, and the cells have receptors that allow them to use this hormone to grow. Treatment with endocrine therapy blocks the growth of the cancer cells.
Hormone receptor (HR) negative. This type of cancer doesn't have hormone receptors, so it won't be affected by endocrine treatments aimed at blocking hormones in the body.
What is the genetic makeup of your breast cancer cells?
Doctors are just beginning to understand how the individual DNA changes within cancer cells might one day be used to determine treatment options. By analyzing the genes of cancer cells, doctors hope to find ways to target specific aspects of the cancer cells to kill them.
A sample of your tumor tissue from a biopsy procedure may be tested in a laboratory to look for:
HER2 gene. Cancer cells that have too many copies of the HER2 gene (HER2-positive cancers) produce too much of the growth-promoting protein called HER2. Targeted therapy drugs are available to shut down the HER2 protein, thus slowing the growth and killing these cancer cells.
Other tumor markers. Researchers are studying ways to interpret the genetic makeup of tumor cells. Doctors hope this information can be used to predict which cancers will spread and which may need aggressive treatments. That way, women with relatively low-risk breast cancers may avoid aggressive treatments.
Tests that analyze the genetic makeup of breast cancers are available but aren't recommended in all situations. Ask your doctor whether this type of test might be helpful in your case.
Doctors are increasingly using genetic information about breast cancer cells to categorize breast cancers. These groups help guide decisions about which treatments are best. Breast cancer groups include:
Group 1 (luminal A). This group includes tumors that are ER positive and PR positive, but negative for HER2. Luminal A breast cancers are likely to benefit from hormone therapy and may also benefit from chemotherapy.
Group 2 (luminal B). This type includes tumors that are ER positive, PR negative and HER2 positive. Luminal B breast cancers are likely to benefit from chemotherapy and may benefit from hormone therapy and treatment targeted to HER2.
Group 3 (HER2 positive). This type includes tumors that are ER negative and PR negative, but HER2 positive. HER2 breast cancers are likely to benefit from chemotherapy and treatment targeted to HER2.
Group 4 (basal-like). This type, which is also called triple-negative breast cancer, includes tumors that are ER negative, PR negative and HER2 negative. Basal-like breast cancers are likely to benefit from chemotherapy.
Understanding more about the chemical and genetic makeup of your cancer may help doctors choose the most effective treatment for your specific cancer.
Tuesday, April 24, 2018
What Are Triple Negative and HER-2 Negative Breast Cancer?
A triple negative breast cancer cell undergoing retraction and apoptosis (cell death) after medical treatment.
Alamy
Triple negative and HER-2 negative breast cancers lack certain receptors that contribute to cancer growth. Receptors are proteins found inside and on the surface of cells that receive messages from substances in the bloodstream telling them what to do. (1)
Because many therapies used to treat the more common types of breast cancer target these receptors, these therapies may not work for triple negative and HER-2 negative breast cancers. This can make finding an effective treatment for these subsets of breast cancer more challenging.
The good news is that there are options available, and researchers are working on finding new medicines to target both triple negative and HER-2 negative cancers.
Triple Negative Breast Cancer Lacks Three Key Receptors
Triple negative breast cancer means that the cells in your tumor don’t contain the three most common types of receptors, which are:
Because triple negative breast cancers lack these receptors, typical medicines that target estrogen, progesterone, and HER-2 are ineffective.
Between 10 percent and 20 percent of breast cancers are triple negative. Younger people, Hispanics, African-Americans, and those with a BRCA1 gene mutation are more likely to develop this type of disease. (2)
Triple negative breast cancers are prone to being aggressive. But every case is different, and your prognosis will depend on many factors. (2)
Basal-like tumors have cells that resemble the basal cells that line the breast ducts. Experts believe that most basal-like breast cancers are triple negative. (1)
HER-2 Negative Breast Cancer Is Missing the HER-2 Protein
HER-2 negative breast cancers have cells that contain little or none of the HER-2 protein.
Women with HER-2 negative breast cancer won’t benefit from therapies that target the HER-2 protein, such as the well-known medication Herceptin (trastuzumab). (3)
Knowing your HER-2 status is important, because this information will determine your treatment options.
Studies have shown that some breast cancers that are HER-2 positive can develop into HER-2 negative cancer, and vice versa. It’s also possible that HER-2 test results can come back wrong, so you might want to get evaluated more than once. (4)
Generally, HER-2 positive breast cancers tend to be more aggressive than HER-2 negative breast cancers. (4)
Testing for Triple Negative and HER-2 Negative Cancers
Your doctor can let you know if you have triple negative or HER-2 negative cancer by testing your receptor status.
Typically, this is done with a biopsy. During a biopsy procedure, a surgeon removes a small amount of tissue and sends it to the lab to be analyzed.
A pathologist will examine the tissue and determine its hormone receptor status. Other tests will also be performed to see if it’s HER-2 positive or HER-2 negative. (5)
Treatments and the Treatment Dilemma
If you have triple negative or HER-2 negative breast cancer, many commonly used therapies may not help your disease. If your cancer is HER-2 negative but not triple negative, you are still a candidate for endocrine therapy typically used to treat breast cancer. If your tumor is HER-2 negative and triple negative, there are still treatments available to help your particular type of breast cancer.
Women with triple negative cancer are usually candidates for chemotherapy, surgery, and radiation. In fact, this type of breast cancer may respond better than other types to chemo if it’s treated early on.
Newer therapies, such as PARP inhibitors, VEGF inhibitors, and EGFR-targeted treatments, are also showing promise in helping women with metastatic triple negative breast cancer in clinical trials. (6)
Surgery, chemo, hormone therapies, and some targeted treatments may be options for those with HER-2 negative breast cancer. (3)
Talk to your doctor about what treatments are most effective for your type of cancer.
Clinical Trials for HER-2 Negative and Triple Negative Breast Cancer
Some women with triple negative and HER-2 negative breast cancers choose to partake in clinical trials to test therapies that aren’t yet available to the public. Additionally, clinical trials help researchers determine whether new treatments are safe and effective.
You may want to consider participating in a research study if your cancer isn’t responding to therapy or has spread to other areas of your body. (7)
Each person is different, and your doctor will likely run several tests before giving you a formal prognosis.
Generally, women with HER-2 negative breast cancers have a better outlook than those with HER-2 positive breast cancers. HER-2 positive cancers are known to grow faster, spread more quickly, and come back more often. Despite this, HER-2 positive breast cancer treatment outcomes have improved dramatically with the approval of drugs like Herceptin (trastuzumab) and Perjeta (pertuzumab). (5)
On the other hand, survival rates tend to be lower for those with triple negative breast cancer. One 2007 study that looked at more than 50,000 patients with different stages of breast cancer found 77 percent of women with triple negative cancer survived at least five years, compared with 93 percent of those with other forms of breast cancer. (1)
Another study, of more than 1,600 women, found that those with triple negative breast cancer had a higher risk of death within the first five years of diagnosis, but not after that time. (1)
Coping With a Less-Common Diagnosis
Receiving a breast cancer diagnosis can be scary, especially when you hear that your type of cancer may not benefit from standard therapies.
Here are some ways you can cope:
Learn about your cancer. Staying informed about your type of cancer can help you make treatment decisions. Ask your doctor about suitable resources for information. The American Cancer Society and the National Cancer Institute are good places to start.
Focus on yourself. A healthy diet, daily exercise, and a good night’s rest are important habits that can equip your body for fighting cancer. Relaxation techniques like yoga and meditation can also help lower your stress levels.
Ask for help. Don’t try to fight cancer on your own. Ask family members or friends to help with household chores, rides to appointments, or managing paperwork.
Join a support group. If you don’t have family or friends nearby, a support group can be a great way to connect with others. Many organizations offer online or in-person support groups. The Triple Negative Breast Cancer Foundation’s online discussion forums give women 24/7 access to support.
More support is needed to help breast cancer patients and survivors manage 'chemobrain' symptoms, such as memory loss, short attention span and mental confusion, according to a study led by researchers from the National University of Singapore (NUS). The study involving 131 female breast cancer patients in Singapore revealed that almost half had suffered from cognitive decline at some point during treatment and up to one year post-treatment. Close to 30 per cent had reported some degree of cognitive impairment one year after undergoing chemotherapy. "Cognitive impairment among breast cancer survivors is an important issue now because early stage breast cancer is treatable. Knowing when patients experience these cognitive problems, and how long the symptoms persist, can aid the development of suitable screening and clinical management measures," said research team leader Associate Professor Alexandre Chan, who is from the Department of Pharmacy at NUS Faculty of Science. Cognitive challenges affecting breast cancer patients Breast cancer is the most prevalent cancer among Singaporean women. Between 2010 and 2014, more than 1,800 women in Singapore were diagnosed with the condition each year. While current treatments convey excellent survival benefits - with more than 90 per cent of patients surviving beyond five years - many patients acquire cognitive toxicities known as chemobrain. These toxicities can dramatically affect patients' quality of life. "Early treatment for breast cancer patients usually involves intensive therapy - this means that patients are exposed to high levels of chemotherapy drugs, and they are also at higher risk of long-term side effects. After treatment, we need to manage survivorship issues. However, the clinical presentation of cognitive toxicities remain poorly understood," explained Assoc Prof Chan. To examine the impact of chemobrain on breast cancer patients, Assoc Prof Chan and his team studied patients with Stages I to III breast cancer. The patients were evaluated at four time points - prior to the start of chemotherapy; six weeks after chemotherapy started; 12 weeks after chemotherapy started; and approximately 15 months after the start of chemotherapy. Both subjective and objective measures were used to assess cognitive decline. For the former, patients were asked whether they faced difficulty in areas such as concentration, memory, multitasking and verbal fluency, using a validated questionnaire. The patients were also evaluated on their attention, memory, mental processing speed and speed of response using a computer-based software. The researchers found that almost half of the respondents suffered from some degree of cognitive impairment during treatment and up to one year post-treatment. About 30 per cent complained of cognitive impairment one year after chemotherapy. In addition, a year after undergoing chemotherapy, 15 per cent of the participants were objectively assessed to suffer from memory challenges, and close to 10 per cent experienced issues with response speed. These results were first reported in the journal Psychooncology earlier this year. Breast cancer survivor Ms Chan Yoke, who is a graphic designer, can attest to cognitive impairment as a result of chemotherapy. In 2015, Ms Chan went through 16 sessions of chemotherapy, along with radiotherapy, as part of her treatment for breast cancer. She said, "I became forgetful after chemotherapy started. I would walk from the kitchen to a room to get something, but once I reached the room, I would not able to recall what I wanted." About three years after the start of her chemotherapy, Ms Chan still grapples with the after-effects of her cancer treatment. She shared that her memory did not go back to what it was like before she had cancer, and her thought processes are also slower than they were prior to the start of her chemotherapy treatment. Early screening and intervention programmes needed The results of this study draw attention to the difficulties faced by breast cancer survivors after completion of active treatment, when they begin to resume their societal roles. The findings also highlight the importance of raising awareness about cognitive impairment among breast cancer patients, so that they can be better prepared for the changes they will experience during treatment and survivorship. "A well-rounded holistic survivorship programme will be very useful for cancer patients and survivors. More importantly, we should actively screen and manage patients at risk of cognitive impairment. This is extremely important as we are expecting to see an increasing number of cancer survivors in Singapore, and cognitive impairment can bring significant negative impact to survivors' quality of life," said Assoc Prof Chan. Researchers from the National Cancer Centre Singapore and KK Women's and Children's Hospital also contributed to the study, which was conducted from 2011 to 2017.
Building on the knowledge gained from this study, Assoc Prof Chan and his team are studying the biomechanisms behind post-chemotherapy cognitive impairment. The researchers will also evaluate the effectiveness of various interventions for managing chemobrain symptoms
Dr. Wachter is a hospitalist, a physician who cares for patients in hospitals and studies how to make hospitals safer and more efficient.
Image
CreditJun Cen
I frequently care for patients with advanced cancer. A majority have already tried some combination of surgery, chemotherapy and radiation. Many have landed back in the hospital because the cancer has returned or spread widely and left them in intractable pain or struggling to breathe.
The hospital stay is often a time when patients decide to stop aggressively fighting their cancer, and instead to focus on palliative care and achieving a measure of comfort and grace at the end of life. The moment of transition can be subtle. It’s sometimes signaled by a sweet look from a husband to a wife, a gentle touch of the patient’s hand by an adult child, or two simple words: “It’s time.”
Over the past 20 years, evidence has demonstrated that palliative care decreases pain, improves comfort and even, in some cases, prolongs life a few months. In my experience, conversations about turning to it often begin with patients recognizing that curing their cancer is impossible. Patients sometimes ask for my opinion on this. While the conversation is often heartbreaking, it has rarely been a hard call.
But now it is. And that has thrown a wrench into the way we treat patients with advanced cancer.
The reason is a new generation of cancer treatments that have become available in recent years. Some, called immunotherapy, harness the patient’s own immune system to battle a tumor. Others, known as targeted therapies, block certain molecules that cancers depend on to grow and spread. The medical literature — usually circumspect when it comes to cancer, in light of many overhyped treatments in the past — now fairly gushes with terms like “revolutionary” and “cure.” In this case, the hype feels mostly justified.
Much has been written about the promise of these treatments, as well as their staggering costs — many cost several hundred thousand dollars a year. But what strikes me most about them is that by blurring the line between cure and comfort — and between hope and hopelessness — they have disrupted the fragile equilibrium that we doctors have long taken for granted.
I recently cared for a woman in her 80s, clearly dying of lung cancer. Or so I thought. “But what about immunotherapy?” her family wondered. When I reluctantly asked our oncologist about this, he didn’t scoff. “It could work,” he said quietly, as if not quite believing what he was saying.
Oncologists are seeing patients whose cases they once would have pronounced hopeless experience Lazarus-like responses to these new therapies. One of my hospital’s specialists in multiple myeloma, a bone marrow cancer with a previously dismal prognosis, recently told me that he had treated a patient with a new kind of immunotherapy. “I think I cured my first case of myeloma,” he said. His voice was filled with awe.
This, of course, sounds like wonderful news for patients and their loved ones. And if these new treatments worked most of the time, this would be an unambiguously happy story. But they don’t.
A recent analysis estimated that about 15 percent of patients with advanced cancer might benefit from immunotherapy — and it’s all but impossible to determine which patients will be the lucky ones. Just last week, a study of lung cancer patients demonstrated the overall benefits of combining immunotherapy with traditional chemotherapy. But here, too, the researchers noted that most patients will not respond to the new treatments, and it is not yet possible to predict who will benefit. In some cases, the side effects are terrible — different from those of chemotherapy but often just as dire.
With patients and family members primed to hold onto every reed of hope, even a small chance of cure or prolonged remission will cause the majority to stick with their pugilistic approach to cancer. In our dichotomous system — one that forces patients to choose between the goal of comfort or cure — this means that most of them will forgo palliative care. We already know that despite the unquestioned value of hospice, many patients with end-stage cancer don’t take advantage of it, or do so with only a few days left in their life, having needlessly suffered for weeks or months. Our new uncertainty will probably make this worse.
What can we do to alleviate this? First, it turns out that many patients can benefit from palliative approaches even as they continue aggressive treatment for their cancer. In 2016 the American Society of Clinical Oncology recommended that concurrent care — palliative and active cancer care delivered at the same time — be made available to patients with advanced cancer. Rules that force patients to choose one approach or another, particularly those that tie insurance coverage of palliative care or hospice to stopping active cancer treatments, should be scrapped.
Second, doctors need more training in how to have these hard conversations with patients in light of the new cancer treatments. Doctors will need to become more at ease with the prognostic ambiguity and better versed in the possible benefits and harms of the new therapies.
Finally, through the federal Cancer Moonshot program, the government is spending hundreds of millions of dollars to study immunotherapy and other emerging treatment options for cancer. The sooner we can work out which patients will — and just as important, won’t — benefit from these approaches, the better.
Sadly, for some patients, a cure will prove elusive. As we continue to chase progress in cancer, let’s be sure that we don’t rob dying patients of a smaller, more subtle miracle: a death with dignity and grace, relatively free from pain and discomfort.
Robert M. Wachter is a professor and chairman of the department of medicine at the University of California, San Francisco.
Chemotherapy Stories: Hear from Real Breast Cancer Patients
Real Women Share their Experiences
Chemotherapy is not a one-size-fits-all experience. When faced with chemotherapy, many women turn to online research, but reading about the treatment and the process only goes so far. Oftentimes, talking with other patients or survivors can be more helpful.
Thirty-seven real women who chose to undergo chemotherapy were interviewed for this article. While none of these women escaped unscathed, they all made it through the treatment and related side effects. Their insights, wisdom, and even humor can provide clarity and hope to those just beginning the chemotherapy journey or to those who are uncertain about the realities of treatment.
Expectations and Preconceptions About Chemotherapy
“I expected to be sicker but the anti-nausea drugs I took made my chemo tolerable.”
“I feared that I would be nauseous and vomit continuously. That did not happen. I had mild nausea only.”
“I didn’t really know what to expect. The biggest challenges were tiredness, nausea, [and] chemo brain.”
Takeaway
Although there are general or typical reactions you can anticipate during chemotherapy, everyone reacts to the treatment differently. Your expectations and ideas may not be what actually happens.
Recommendations
Speak openly with your oncologist and learn about your individual treatment plan, including the chemotherapy drugs and other medications you will be taking. Ask what you should do to help prevent side effects, how to manage any side effects you have, and what side effects you should report.
“The biggest challenge was to accept my limitations and learn to be dependent on others.”
“I had to plan to do only one thing each day, like cook dinner.”
“Chemo and recovering became the primary focus in my life, followed by enjoying my good weeks with friends and family.”
Takeaway
Chemotherapy can be draining, both physically and mentally. For women who are used to being self-sufficient, learning to accept help from friends and family can be difficult. Just remember: You’re undergoing the treatment in the hope of returning to your strong, capable self.
Recommendations
Listen to your body. You may feel the urge to push through and continue with your normal schedule, but being too active may affect your recovery period. Get enough rest and make sure to fuel your body. Proper nutrition is necessary during recovery. The American Cancer Societyrecommends eating more lean proteins, like fish, poultry, and low-fat dairy. These items are necessary to help heal healthy tissues from damaging chemotherapy and also fight infections.
“The most bothersome side effects were ones I had not expected.”
“The list of side effects they give you is SO long, but you really don't know what it will be like…Everyone is different and responds differently.”
“I would be so exhausted I could hardly drag myself out of bed.”
Takeaway
As much as you try to prepare yourself for common side effects such as fatigue, weakness, hair loss, and nausea, your experience may be very different from what you expected. Some side effects, such as dry mouth and diarrhea, are not as noticeable to outsiders and are therefore not as widely discussed. Your body is unique, so how it responds will also be unique.
Recommendations
After your first treatment, you’ll quickly find out how your body is reacting to the treatment. If you’re having a difficult time, let your cancer team know. They can probably help mitigate difficult side effects. It’s also important to talk with your family and loved ones before and during your treatments about how you’re feeling. Having a strong support system can help you recuperate.
“I knew I'd lose my hair and be very ill. I did not realize that most women gain weight during chemo.”
“Losing my hair made me having cancer very visible.”
“Chemo aged me. My eyes had dark circles, but my skin actually cleared up a bit.”
Takeaway
Hair loss may be one of the most familiar side effects, but that doesn’t make it less traumatic. You may also experience other changes in your physical appearance, such as weight gain or loss.
Recommendations
The American Cancer Society’s Look Good Feel Better class offers women the opportunity to try a new look by experimenting with wigs, hats, and scarves. Women also learn makeup tips and tricks.
“Before chemo, I wanted to be superwoman and bounce back super quick. I wanted to be the one with no negative side effects, who could hold it all together.”
“My supervisor was wonderful and wasn’t strict with how much time I needed off. But I continued to work all through chemo.”
“My immediate team was aware of the treatment and compensated for the fact that I was physically there 100 percent of the time but only working to about 50 percent of my usual capacity.”
Takeaway
The reality is you can’t control how your body is going to react to chemotherapy. Many women have to pull back and aren’t able to continue working as before.
Recommendations
Listen to your body. It will tell you what it needs. Talk to your boss, manager, or HR department to discuss a lighter work schedule.
“The experience made my relationships with my husband, parents, and a couple of friends stronger. I always had someone there with me.”
“Once chemo started, I thought, ‘I can't do this. I'd rather die of cancer. This has GOT to be worse.’ Then my 5-year old came home, bubbling with life and love, and I realized that I had to try. He needs his mommy.”
“I hated people treating me like I was sick. On the positive side, it definitely strengthened my relationships with close family and made me appreciate my close friends and colleagues more.”
Takeaway
Sometimes your loved ones can be the best support system. You may find they can provide you with the strength to push through the hard times.
Recommendations
Even if you’re blessed with having a strong family and friend network, having an outside support group can be beneficial. It’s helpful to talk to others who have gone through, or are going through, a similar experience. Ask your cancer team about a support group in your area or join one online.
“I’m still experiencing side effects almost a year later. I hope that goes away soon.”
“I found out how strong I really am.”
“The thing that surprised me the most was that chemotherapy, while no walk in the park, was not as bad as I expected.”
Takeaway
Not knowing what’s ahead or what to expect can be scary. Some women may become frustrated by the unexpected. Others may discover something about themselves that’s inspirational.
Recommendations
While preparing for the unknown may be impossible, anticipating that there will likely be bumps, delays, and roadblocks during your treatment and recovery can make dealing with them less stressful. Being patient with yourself and spending time reflecting on your needs can be helpful.
“It was not what I imagined, but I would do it again if I found out I had cancer again.”
“Until you do the chemo, it is hard to imagine the fatigue.”
“It’s doable and manageable with all the anti-nausea/anti-anxiety drugs available.”
Takeaway
Chemotherapy isn’t easy, but it can be manageable. With advances in medicine and research, you have more options and choices than ever before to make the treatment less miserable.
Recommendations
Remember that you’re not alone. Women just like you have gone through the same journey. Hearing and listening to them may make the process less scary or wearisome.
















.jpeg)

